

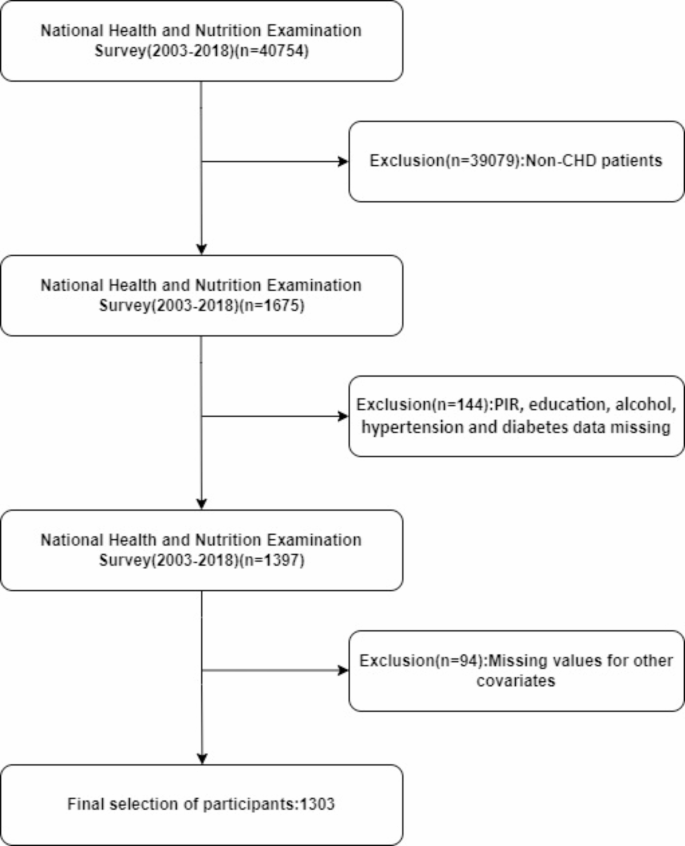
NHANES study population
Participants were excluded based on several criteria:1 being under 18 years of age;2 missing data on DII or mortality. Additionally, those lacking information on variables such as education level, marital status, poverty-income ratio (PIR), BMI, and laboratory data were also excluded. Ultimately, 1303 eligible patients were selected. Figure 1 illustrates the specific research process. The NHANES conducts cross-sectional studies to assess the general health and nutritional status of the non-institutionalized U.S. population20. The NHANES protocol received approval from the Ethics Review Committee of the National Center for Health Statistics (NCHS), and all participants gave written informed consent. Given the public accessibility and the nature of NHANES data, the Ethics Committee of the Second People’s Hospital of Hefei waived the need for ethical approval for this study.
Definition of CHD
The diagnosis of CHD relies primarily on disease history21. Participants confirmed their CHD status in the health questionnaire by answering whether a doctor or other health professional had diagnosed them with CHD.
Death-related information
This study reported all-cause and CVD mortality. Mortality data from NHANES (2003–2018) were linked with death certificates from the National Death Index using a probability matching algorithm to ascertain mortality status. CVD mortality was determined by ICD-10 codes I00-I09, I11, I13, I20-I51, and I60-I69. Follow-up concluded upon the patient’s death or on December 31, 2019.
Meal validation index
Dietary intake was recorded using the 24-hour dietary recall method, and the DII was calculated following the method developed by N. Shivappa et al.14. Dietary data were validated using the Nutrition Data System for Research (NDSR)22. In this study, 28 dietary variables were utilized to calculate the DII, including carbohydrates, protein, total fat, alcohol, fiber, cholesterol, saturated fatty acids, monounsaturated fatty acids, polyunsaturated fatty acids, n-3 fatty acids, n-6 fatty acids, niacin, vitamins A, B1, B2, B6, B12, C, D, E, and minerals such as iron, magnesium, zinc, selenium, along with folate, β-carotene, caffeine, and energy. Previous studies have demonstrated the DII’s consistent predictive ability with these 28 dietary components23.
Covariates
Based on prior research and clinical experience, factors associated with CHD mortality were included: age, gender, race, educational attainment, marital status, poverty-income ratio (PIR), diabetes, hypertension, body mass index (BMI), smoking, and alcohol use. Race categories were defined as non-Hispanic black, non-Hispanic white, Mexican American, and other. PIR was categorized into three levels: < 1.0, 1.0–3.0, and > 3.0. Marital status was classified into married, divorced, unmarried, and other. Educational levels were divided into below high school, high school or equivalent, and college or higher. Smoking status was categorized into:1 never smokers, defined as those who smoked fewer than 100 cigarettes in their lifetime;2 former smokers, defined as those who smoked 100 or more cigarettes in their lifetime but no longer smoke;3 current smokers, who smoke on some days or daily. Alcohol intake was categorized into never, former, heavy, moderate, and mild drinkers. BMI was calculated by dividing weight (kg) by height squared (m2), with categories of normal (< 25 kg/m2), overweight (25 ≤ BMI ≤ 30 kg/m2), and obese (BMI > 30 kg/m2). Laboratory tests included Alanine aminotransferase (ALT), Aspartate aminotransferase (AST), albumin, neutrophils, lymphocytes, hemoglobin, glycated hemoglobin (HbA1c), creatinine, uric acid, and blood urea nitrogen (BUN).
Statistical analysis
Data analysis was conducted using R software (version 4.3.2, The MEC sample weight (WTMEC2YR/8) was used for weighted analysis of the data. Continuous variables were presented as means (SE), and categorical variables as frequencies (%). Spearman’s rank correlation coefficient was employed to assess the correlations between continuous variables.
The relationship between the DII and all-cause mortality risk in CHD patients was explored using a multivariable Cox proportional hazards regression model. The DII was analyzed as both a continuous and categorical variable, categorized into pro-inflammatory (DII > 0) and anti-inflammatory (DII < 0) diets, to assess the robustness of the findings. Model 1 was unadjusted, Model 2 adjusted for age, race, and gender, and Model 3 included further adjustments for education level, smoking, alcohol consumption, hypertension, and diabetes, building on Model 2.
Stratified analyses were conducted based on age, gender, race, BMI, hypertension, and diabetes. To ensure the reliability of the results, we performed several sensitivity analyses. First, we excluded CHD patients who had died within the first two years of initial follow-up and reassessed the relationship between DII and all-cause mortality in CHD patients. Second, we performed non-survey-weighted multivariate logistic regression to investigate the relationship between DII and all-cause mortality in CHD patients.The relationship between the DII and all-cause mortality was also examined using RCS analysis, focusing on variations across different genders. A collinearity test was performed, considering a variance inflation factor (VIF) > 10 indicative of collinearity. All statistical methods and results were rigorously checked for accuracy and clarity.
link