

Characteristics of study participants
This section describes the baseline characteristics of the participants. The average age of the participants is 65.85 years, reflecting the aging cohort under study.In terms of basic demographic characteristics, the gender distribution was slightly skewed towards females, who constituted 52.49% of the sample. The majority of participants have a low level of education, primarily at the primary school level or below(79.19%).This educational distribution is critical as it correlates with other socioeconomic factors such as employment in agriculture and living conditions. Most households had a strong familial support structure, as evidenced by 85.26% of household members being married or cohabiting, which may influence health outcomes and care-seeking behaviours.
Regarding household characteristics and other socioeconomic factors, the majority of respondents held rural hukou type(76.10%) and resided in rural areas(61.73%). This status has impacted their access to healthcare services and insurance, potentially posing specific challenges in obtaining medical resources and financial support. The basic medical insurance coverage rate has reached 92.80%, nearing universal coverage.
Table 1 shows the baseline characteristics stratified by chronic disease status. Participants who were older, male, less educated, held urban hukou, resided in urban areas, and had health insurance were more likely to be diagnosed with chronic diseases (all p < 0.05). In our sample, no significant difference was found between marital status (living with a spouse or not) and chronic disease prevalence (p > 0.05).The analysis sample includes a total of 6,483 participants who did not have CHE at baseline.
Figure 2 illustrates the incidence of CHE across the three survey waves in 2015, 2018, and 2020, as well as its distribution based on chronic disease status. Among elderly individuals in China, the incidence of CHE was 12.25% in 2015, increased to 18.73% in 2018, and reached 14.62% in 2020. Elderly individuals with single chronic diseases or multimorbidity had higher CHE incidence rates compared to those without chronic diseases.
Longitudinal relationship between chronic diseases and catastrophic health expenditure
To examine the impact of chronic diseases on catastrophic health expenditure (CHE), this study categorizes chronic disease prevalence into single chronic diseases and multimorbidity. A mixed-effects logistic regression model using panel data is employed to explore the longitudinal impact of chronic diseases on CHE, with results presented as odds ratios (OR) and 95% confidence intervals (CI). Three models are applied hierarchically to address potential confounding factors. Model 1 is a crude model with no adjustments for covariates; Model 2 adjusts for participants’ basic demographic characteristics (age, gender, education attainment and marital status); Model 3 further includes household characteristics and other socioeconomic factors (hukou type, place of residence, and health insurance).
Table 2 reports the stepwise regression results. The study results indicate that in all three models, the occurrence of chronic diseases significantly increases the risk of catastrophic health expenditure, regardless of whether it involves a single chronic condition or multimorbidity. In the crude Model 1, both single chronic diseases(P < 0.001, 95% CI: 1.16–1.44) and multimorbidity(P < 0.001, 95% CI: 1.10–1.36) significantly influence the occurrence of CHE. The results remain similar in Model 2, which adjusts for a few covariates. In the fully adjusted Model 3, both single chronic diseases(P < 0.001, 95% CI: 1.22–1.52) and multimorbidity(P < 0.001, 95% CI: 1.18–1.47) continue to significantly increase the risk of CHE.
The results for other covariates show that age(P < 0.01), education level (p < 0.001), marital status (p < 0.001), hukou(p < 0.001), and residence (p < 0.001) are significantly associated with CHE. Age is an important factor influencing catastrophic health expenditure in elderly households, the older the age, the higher the risk of CHE. Higher education levels reduce the occurrence of CHE. Living with a spouse may increase the risk of CHE. Co-residing couples constitute a larger household unit, potentially leading to higher overall medical needs. Elderly couples living together may both face health challenges, increasing the likelihood of incurring substantial medical costs. Compared to urban elderly households, rural elderly households are more prone to experiencing CHE. Notably, our data analysis indicates that basic medical insurance has no significant impact on CHE, suggesting that the current basic medical insurance system is insufficient to mitigate the risk of CHE for households. These findings highlight the substantial financial burden that chronic health conditions and other adverse circumstances can impose on families.
Detailed statistical results are presented in Table 2, illustrating the longitudinal impact of various variables on the likelihood of CHE occurrence within the cohort.
Stratification Analyses.
Stratification analysis
We further conducted stratified analyses to examine whether the impact of chronic diseases on catastrophic health expenditure (CHE) varies across different demographic subgroups, as illustrated in Fig. 3 The forest plot indicates that, after adjusting for covariates such as key demographic characteristics, the presence of chronic diseases is associated with a higher likelihood of CHE. This pattern of effect was consistently observed across various subgroups, including those defined by gender, education level, marital status, hukou type, place of residence, and health insurance. Furthermore, the interaction terms between the aforementioned covariates and chronic disease status were not statistically significant (all p-values for interaction > 0.05).
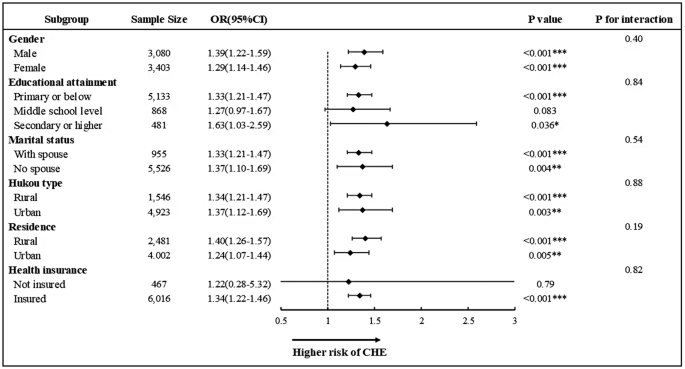
Association between chronic diseases and CHE across different subgroups. The forest plot depicts the longitudinal association between chronic diseases conditions and CHE across different covariate subgroups. All models were adjusted for a predefined full list of covariates (including age, gender, education, marital status, hukou type, place of residence and health insurance) except the stratification variable. (*p < 0.05, **p < 0.01, ***p < 0.001; 0R, odds ratio; CI, confidence interval)
Sensitivity analysis
To ensure the robustness of our findings, sensitivity analyses were conducted using two methods. First, considering the heavy economic burden imposed by cancer, we excluded participants diagnosed with cancer and repeated the above analysis using a fully adjusted model. The results, as shown in Table 3, indicate that after excluding cancer patients, chronic disease prevalence still significantly impacts catastrophic health expenditure.
The second sensitivity analysis was conducted by classifying catastrophic health expenditure using different thresholds.According to the definitions provided by the WHO and the World Bank, catastrophic health expenditure is defined in three ways: if out-of-pocket (OOP) healthcare expenditure equals or exceeds 10% and 25% of total household consumption expenditure, and 25% of total non-food household consumption expenditure. The consistency of results across these varying thresholds confirms the reliability of our main findings and suggests that our conclusions about the impact of chronic diseases on CHE are stable regardless of the specific threshold applied.
Additionally, through sensitivity analyses using different thresholds, we found that when CHE was defined as equal to or exceeding 40% of total non-food household consumption expenditure—a relatively high threshold—the likelihood of experiencing CHE increased by 36% and 32% for households with single chronic conditions and those with multiple chronic conditions, respectively, compared to households without chronic conditions. Notably, the impact of a single chronic condition on CHE surpassed that of multiple chronic conditions under this higher threshold. However, when applying the other three lower thresholds, the economic burden became more pronounced for households with multiple chronic conditions.
The outcomes of these sensitivity analyses are documented comprehensively in Table 4, providing a transparent view of how varying definitions of CHE affect the analysis.
link