

During data collection, 203 individuals consented to participate in the study. Following screening based on inclusion and exclusion criteria, 17 participants were excluded because they did not meet the age requirement, had uncontrolled medical conditions, or declined to continue, leaving 186 eligible participants. However, 4 individuals were further excluded from higher-PA group and 6 from lower-PA group due to incomplete filling of questionnaires or unable to complete the objective assessments or decline to participate. Consequently, the final analysis included 176 participants, evenly distributed between the lower- and higher-PA groups (n = 88 per group; Fig. 1).
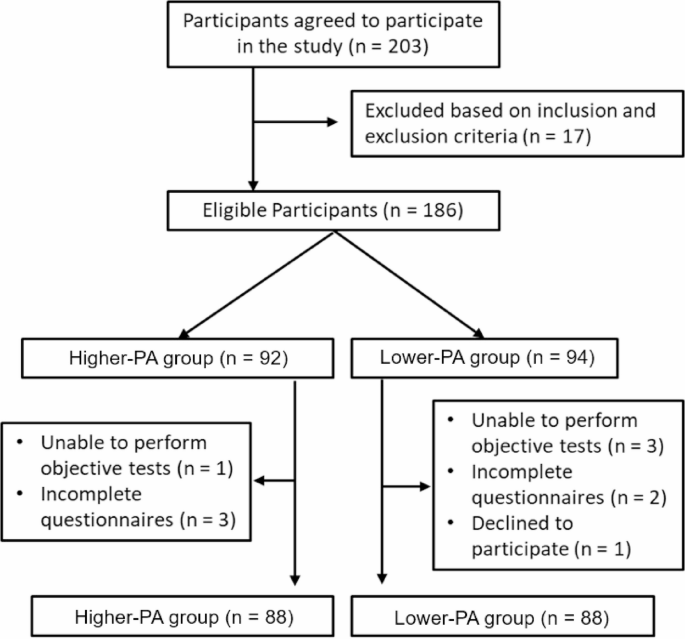
Flow of participants through the study. PA; Physical Activity
Table 1 describes the baseline sociodemographic characteristics of the participants. Almost two-thirds were male and married (n = 136, 77.3%). Most participants were aged 60–64 years (n = 78, 44.3%), had completed high school education (n = 92, 52.3%), and reported an average monthly income (n = 94, 53.4%). Thirty-four (19.3%) participants reported falls in the past year, with injuries occurring in 26 (14.8%) cases.
Table 2 compares all outcomes between the higher-PA group and the lower-PA group. The higher-PA group demonstrated significantly lower TUGT, 5xSTST, 10MWT, and FES-I scores than the lower-PA group. The 2MWT, mCTSIG-Tol, and all domains of the WHOOL-BREF were significantly greater for the higher-PA group than the lower-PA group. These results indicated that the higher-PA group had better physical performance, less FoF, and better QoL in all domains than the lower-PA group.
Significant differences in multiple physical performance outcome measures were observed when compared between different sociodemographic groups (Table 3). The TUGT revealed significantly slower performance among females than males, with younger participants (60–64 years) significantly outperforming older groups. In the 2MWT, males covered a significantly greater distance than females, with younger participants (60–64 years) achieving the highest distances compared to older groups. Likewise, 10MWT showed males were significantly faster than females, and younger participants significantly outperformed older groups. Active individuals had significantly higher mCTSIB scores than the lower-PA group, while females and older participants exhibited poorer balance.
Table 4 compares the FoF, sleep, and QoL between different sociodemographic groups. FES-I scores were notably higher in the 70–74 age group and among housewives compared to their counterparts. Those sleeping < 7 h/night had higher FES-I scores than those sleeping ≥ 7 h. Participants with a history of falling had significantly higher FES-I score than those without. Individuals aged 70–74 years had significantly higher PSQI scores among age groups. Participants with a middle school education had significantly the highest PSQI scores among their group. Workers or farmers had notably higher scores than other professions. Individuals who experienced falls or fall-related injuries in the past year demonstrated significantly higher PSQI scores than their counterparts. Nightly sleep duration below 7 h also corresponded to poor sleep quality. Figure 2 illustrates the proposed mediation model examining the relationship between physical activity level and quality of life (QoL). In this framework, balance (mCTSIB), functional capacity (2MWT), lower extremity strength (5xSTS), fear of falling (FES-I), and sleep quality (PSQI) act as potential mediators. The model hypothesizes that physical activity enhances these health-related factors, which in turn contribute to improved QoL. Pathways a and b represent the indirect effects through mediators, while path c′ denotes the direct effect of physical activity on QoL after accounting for mediation.

Conceptual mediation model showing how physical activity level may influence quality of life (QoL) via simple health-related mediators: balance (mCTSIB), functional capacity (2MWT), lower extremity strength (5xSTS), fear of falling (FES-I), and sleep quality (PSQI). Paths a and b indicate indirect effects, while path c′ represents the direct effect controlling for mediators
The simple mediation analyses (Model 4) assessing whether functional mobility tests and mCTSIB total score, as well as psychological measures [FES-I and PSQI global score] mediate the association between physical activity levels and four domains of QoL as measured by the WHOQOL-BREF. Across the domains, significant total effects of physical activity levels were observed on WHOQOL-PH (β = 2.375, p =.001), WHOQOL-PS (β = 2.263, p =.003), WHOQOL-SR (β = 1.812, p =.014), and WHOQOL-EH (β = 1.932, p =.006).
The direct effects of PA levels remained statistically significant for all domains when controlling for each mediator individually, although the magnitude was reduced compared to total effects, indicating partial mediation in most cases.
Among the mediators, the 2MWT consistently demonstrated statistically significant indirect effects across WHOQOL-PH (β = 0.612, p =.002), WHOQOL-PS (β = 0.537, p =.005), WHOQOL-SR (β = 0.438, p =.010), and WHOQOL-EH (β = 0.422, p =.012), suggesting that walking endurance partially mediates the relationship between physical activity levels and overall QoL.
Similarly, TUGT was a significant mediator for WHOQOL-PH (β = 0.576, p =.003), WHOQOL-PS (β = 0.493, p =.006), WHOQOL-SR (β = 0.407, p =.014), and WHOQOL-EH (β = 0.401, p =.017), indicating the relevance of dynamic balance in this association.
The FES-I mediated the effects of physical activity levels on WHOQOL-PH (β = 0.520, p =.007), WHOQOL-PS (β = 0.486, p =.009), and WHOQOL-SR (β = 0.375, p =.020), while the PSQI mediated the relationships with WHOQOL-PS (β = 0.432, p =.011), WHOQOL-SR (β = 0.387, p =.015), and WHOQOL-EH (β = 0.475, p =.009).
The mCTSIB total score was a significant mediator for WHOQOL-PH (β = 0.439, p =.011) and WHOQOL-PS (β = 0.391, p =.017).
The mediation type was classified as partial for all significant paths due to the persistence of a significant direct effect in each case. Full details, including unstandardized coefficients, 95% confidence intervals, and exact p-values for each total, direct, and indirect effect, are provided in Table 5.
We initially examined each potential mediator separately, then fit a parallel mediation model to evaluate their unique contributions. A parallel mediation analysis was used to evaluate the indirect effects of physical activity levels on four domains of WHOQOL-BREF. This parallel framework allows for the estimation of each indirect path while controlling for all other mediators in the model.
In the WHOQOL-PH domain, significant indirect effects were observed through 2MWT (β = 1.032, p =.001), 10MWT (β = 1.116, p =.003), mCTSIB (β = 0.401, p =.006), and PSQI (β = 1.099, p =.001), suggesting partial mediation. For WHOQOL-PS, TUGT (β = 0.659, p =.006), 10MWT (β = 0.806, p =.005), mCTSIB (β = 0.514, p =.006), FES-I (β = 0.651, p =.002), and PSQI (β = 1.061, p =.001) showed significant parallel mediation effects.
In the WHOQOL- SR domain, 2MWT (β = 0.546, p =.006), mCTSIB (β = 0.357, p =.015), FES-I (β = 0.492, p =.001), and PSQI (β = 0.592, p =.001) demonstrated statistically significant indirect effects. For WHOQOL-EH, a significant indirect effect was observed only through FES-I (β = 0.475, p =.002), with other mediators showing non-significant effects.
A parallel mediation model evaluating the direct and indirect effects of physical activity levels on the QOL domains score, mediated through seven functional and psychosocial variables, while adjusting for age group, gender, marital status, education level, income, and occupation.
The total effect of physical activity levels on WHOQOL-PH was statistically significant, b = 1.55, SE = 0.61, t = 2.54, p =.01, with a standardized coefficient (β) of 0.36. Upon inclusion of mediators, the direct effect was attenuated and became non-significant (β = 0.97, SE = 0.60, p =.11), suggesting partial mediation.
Among the mediators, FES-I and PSQI were significant predictors of WHOQOL-PH. FES-I exhibited a negative and statistically significant effect on QoL (β = − 0.16, SE = 0.04, p <.001), with a standardized coefficient of –0.30. PSQI also showed a negative association (β = − 0.30, SE = 0.11, p =.00).
Bootstrapped indirect effects indicated that FES-I was the only statistically significant mediator of the relationship between physical activity levels and WHOQOL-PH, with a point estimate of 0.61, SE = 0.26, and a 95% Cl [0.18, 1.17], not crossing zero. The partially standardized indirect effect through FES-I was also significant (Effect = 0.14, SE = 0.06, 95% CI [0.04, 0.26]).
Other mediators, including TUGT, 5xSTST, 2MWT, 10MWT, mCTSIB, and PSQI, did not demonstrate statistically significant indirect effects, as their 95% CI included zero. The overall total indirect effect was non-significant (Effect = 0.58, SE = 0.41, 95% CI [–0.18, 1.46]).
Overall, the full model explained 42% of the variance in WHOQOL-PH (R² = 0.42, p <.001). Among covariates, gender (β = –0.15, p =.04) remained a significant predictor of the outcome in the adjusted model.
The total effect of physical activity levels on WHOQOL-PS was statistically significant, B = 1.49, SE = 0.64, p =.02, with a standardized effect size of 0.35. However, after controlling for the mediators, the direct effect was attenuated and no longer significant, B = 0.84, SE = 0.61, p =.17, indicating partial mediation.
Among the mediators, only FES-I and sleep quality significantly contributed to the model. Specifically, FES-I showed a significant negative effect on WHOQOL-PS (β = −0.13, p =.00) and a significant indirect effect from PA levels to WHOQOL-PS through FES-I (indirect effect = 0.48, SE = 0.21, 95% CI [0.11, 0.95]). PSQI also exerted a significant negative effect on WHOQOL-PS (β = −0.51, p =.00); however, the indirect effect of PA levels via PSQI was not statistically significant (indirect effect = 0.14, 95% CI [−0.32, 0.60]).
Other mediators, including TUGT, 5xSTST, 2MWT, 10MWT, mCTSIB, did not demonstrate significant indirect effects, with all respective 95% Cl crossing zero. The total indirect effect of physical activity on WHOQOL-PS across all mediators was non-significant (indirect effect = 0.65, 95% CI [−0.17, 1.57]).
Model fit indices for individual mediator equations varied. Physical activity levels significantly predicted better TUGT performance (β = −1.08, p <.001) and faster 10MWT (β = −0.34, p =.02), but not 5xSTST, 2MWT, or mCTSIB. Physical activity levels were significantly associated with lower FES-I score (β = −3.82, p =.00) but not with PSQI (B = −0.27, p =.54).
A statistically significant total effect of PA levels on WHOQOL-SR was observed (β = 0.90, p =.02), which remained significant in the direct effect model (β = 0.92, p =.02), indicating a robust positive relationship between physical activity and social relationships independent of the mediators.
None of the individual or total indirect effects reached statistical significance, as all bootstrap confidence intervals (CIs) included zero. The largest negative indirect effect was observed through 5xSTST (β = −0.13, Boot 95% CI: −0.32, 0.03), and the largest positive effect was via PSQI (β = 0.08, Boot 95% CI: −0.20, 0.36), though both effects were nonsignificant. The total indirect effect was also nonsignificant (β = −0.02, 95% CI: −0.49, 0.41), suggesting that the mediators collectively do not account for a statistically significant proportion of the association between physical activity level and QoL.
Among the mediators, physical activity level significantly predicted better performance in TUGT (β = −1.08, p <.001), 10MWT (β = −0.34, p =.02), 2MWT (β = 2.34, p =.05), and FES-I (β = −3.82, p <.001). No significant effects were found for 5xSTST, mCTSIB, or PSQI. These associations indicate that higher physical activity levels were related to faster mobility, improved endurance, and reduced fear of falling, though these functional improvements did not significantly mediate the effect on WHOQOL-SR.
Age group and occupation showed significant associations across several models. Age was a strong predictor in TUGT (β = 0.88, p <.001), 2MWT (β = −2.28, p <.01), mCTSIB (β = −7.41, p <.001), and FES-I (β = 2.38, p <.01). Occupation was associated with TUGT (β = 0.55, p <.001), FES-I (β = 1.47, p =.01), and PSQI (β = 0.53, p =.02). Education level was inversely related to PSQI (β = −0.55, p <.01), indicating better sleep quality with higher education.
The total effect of physical activity on WHOQOL-EH was statistically significant, B = 1.57, SE = 0.73, p =.03, 95% CI [0.12, 3.02], with a partially standardized coefficient of 0.33. When controlling for all mediators, the direct effect was attenuated and no longer statistically significant (β = 1.36, SE = 0.75, p =.07, 95% CI [− 0.13, 2.84]), suggesting the presence of partial mediation.
Among the mediators, only the 2MWT demonstrated a statistically significant indirect effect (β = 0.50, SE = 0.33, 95% CI [0.01, 1.28]; partially standardized effect = 0.11, 95% CI [0.00, 0.27]), indicating that increased physical activity was associated with better walking endurance, which in turn predicted better scores on the WHOQOL-EH.
All other indirect effects via TUGT, 5xSTST, 10MWT, mCTSIB, FES-I, and PSQI were not statistically significant, as the corresponding bootstrap confidence intervals included zero. The total indirect effect across all mediators combined was non-significant (β = 0.22, SE = 0.42, 95% CI [− 0.62, 1.08]), with a partially standardized total indirect effect of 0.05, 95% CI [− 0.13, 0.23]. The model explained 23% of the variance in the outcome variable (R² = 0.23, F (14,161) = 3.35, p <.001), supporting a moderate overall fit.
Table 6 presents the total, direct, and indirect effects of physical activity levels on each WHOQOL domain, controlling for sociodemographic characteristics.
link