


Abstract
As the global population ages, dental professionals increasingly encounter patients with cognitive impairments that compromise their ability to provide informed consent. This presents complex ethical and legal challenges, particularly in the context of extensive dental treatment. Informed consent is a foundational principle in health care, grounded in respect for patient autonomy and requiring a process that includes capacity assessment, disclosure, understanding, voluntariness, and authorization. However, in geriatric dentistry, the application of these principles is often inconsistent and underexplored. This article reviews the ethical frameworks and regulatory standards that guide informed consent in dentistry, with particular attention to patients who lack decision-making capacity. Drawing on recent literature, the authors highlight the gaps in current practice and the need for clearer guidance and practical tools. A case history is presented to illustrate the dilemmas that arise when treating cognitively impaired patients, emphasizing the importance of shared decision-making, surrogate involvement, and ethical sensitivity in clinical care.
Key-words: informed consent, decision making, dental care, cognitive dysfunction, dementia
The global population is aging, and this demographic shift is reshaping health care systems worldwide.1 As individuals live longer, they are more likely to develop chronic conditions that require long-term care, specialized support, and increased health care resources. Older adults often present with complex medical histories, necessitating providers to understand the oral consequences of these diseases and the medications used to treat them. Consequently, it will need oral health professionals who are trained in geriatrics and gerontology to deliver age-appropriate and effective care.2,3
Despite the predictability of this trend, there remains a very large shortage of health care professionals—particularly in dentistry—who are adequately prepared to meet the needs of aging patients.4,5 A very significant development in dental care is the increasing number of older adults who are retaining their natural teeth.6 These dentitions have often been extensively restored, including large fillings, crowns, implants, and various kinds of dental prosthesis, which are difficult for the older adult to maintain.7 As these individuals age, chronic illnesses and cognitive decline can compromise their ability to maintain an adequate level of daily oral hygiene, leading to rapid deterioration of these dentitions, which require significant dental interventions.8
In such cases, dentists may face the challenges of obtaining informed consent from patients whose decision-making capacity has become impaired—or, in some circumstances, uncertain.9-11 When cognitive impairment is suspected, providers must approach consent discussions with heightened sensitivity to ensure the patient’s rights are respected. It’s essential to confirm that the patient understands the purpose, risks, and benefits of a proposed treatment plan. Signs such as overly quick agreement or refusal, lack of consideration of alternatives, or limited comprehension may indicate impaired decision-making capacity. However, the presence of physical or mental impairments alone does not automatically preclude a patient from giving informed consent. Clinicians should use their professional judgment to assess the patient’s overall functioning. If there is any uncertainty about the patient’s ability to consent, it is best to pause the procedure and seek further evaluation.11 This situation raises a host of ethical questions and practical dilemmas, often with limited guidance available in the dental literature.12 Legal standards for consent vary widely across jurisdictions, and contribute further complexity to clinical decision-making.9,10
Nevertheless, core ethical principles and regulatory frameworks can offer valuable direction.10,12,13 In this article, we examine these principles and guidelines, using a case history to illustrate the nuanced challenges that arise when providing dental care to patients who are unable to give informed consent.
Ethical principles and regulatory frameworks
Informed consent is a foundational ethical and legal principle in health care, including dentistry. It is defined as an autonomous action by which a patient authorizes a health professional to initiate a proposed treatment plan, based on adequate understanding, voluntariness, and without coercion.13 The process is not merely a formality or a signed document, but a meaningful dialogue that respects the patient’s right to self-determination. Historically, it is rooted in response to egregious violations of human rights in medical research during World War II and as a result, the Nuremberg code was developed.13 Accordingly, the doctrine of informed consent has evolved to protect patients’ rights in clinical care and must emphasize the moral imperative to respect individual autonomy. In the dental setting, informed consent serves multiple critical functions: it protects the patient’s autonomy and dignity, prevents coercion or manipulation, encourages thoughtful clinical decision-making, and fosters trust in the dentist–patient relationship. These goals are best achieved through shared decision-making, where patients are supported in understanding their options and making informed choices that align with their values and preferences.11,13
A valid informed consent process in dentistry requires the integration of several key elements that collectively uphold the patient’s autonomy and ensure ethical clinical practice. These elements include: decision-making capacity, voluntariness, disclosure of material information, recommendation, understanding, deliberation, and authorization.10,11 Capacity refers to the patient’s ability to comprehend relevant information, appreciate the implications of their choices, reason through options, and express a clear preference. Voluntariness ensures that the decision is made freely, without coercion or undue influence. Disclosure involves presenting the patient with comprehensive information about the proposed treatment, including risks, benefits, and reasonable alternatives. The clinician’s recommendation helps guide the patient through the decision-making process, which should culminate in a well-informed and deliberate choice. Importantly, this process is best facilitated through shared decision-making, a collaborative model in which clinicians and patients—or their surrogates when capacity is impaired—work together to determine the most appropriate course of care. This approach is especially critical when treating older adults with cognitive impairment, where capacity may fluctuate and ethical complexities often arise.10,11
Despite the centrality of informed consent in ethical dental practice, its application in geriatric dentistry remains underdeveloped and inconsistently implemented. A recent systematic review12 revealed that informed consent in dental care for older adults is rarely studied, with only a handful of publications addressing the topic directly. The review identified significant gaps in how core elements—such as capacity assessment, comprehension, and voluntariness—are operationalized in dental settings. Moreover, the literature suggests that many older adults may defer decision-making to clinicians or family members, either due to cognitive decline or cultural expectations, raising concerns about the authenticity of consent. The review also emphasized the need for practical tools to assess capacity in dental practice and called for greater attention to concepts like geriatric assent, shared decision-making, and the role of surrogates. These findings underscore the urgency of developing more robust, evidence-based frameworks to support ethical decision-making in the care of cognitively impaired dental patients.12
Case scenario
Mrs. MR was 89 years old at her first appointment, and her daughter brought her to us in a wheelchair. She stated that she wanted her mother to have a dental check-up because her mother was only able to eat pureed food and kept rubbing her mouth. Mrs. MR lived in a long-term care facility about one hour away. Mrs. MR daughter was her legal guardian and had durable power of attorney for health and finances.
The long-term care facility supplied the following medical history: Diverticulitis; Alzheimer’s disease diagnosed six years ago; Hiatal hernia not surgically repaired; Left hip replaced eight years ago; Osteoarthritis of her back and hips; Noncommunicative; Sleep problems with sundowning; Squamous cell carcinoma of the palate removed surgically 3 years ago, no follow -up with radiation or chemotherapy; and allergy to penicillin.
Her medication included Haldol 2mg bid (haloperidol), a butyrophenone antipsychotic, which can cause xerostomia, tardive dyskinesia and orthostatic hypotension; Valium 2mg qd (diazepam) a benzodiazepine, which is a tranquilizer that can cause xerostomia, orthostatic hypotension, and increase the risk of falling; Colace 100mg/30mg bid; (docusate salts or dioctyl sulfosuccinate), a laxative, which allows water and fats to get into the stool. This helps soften fecal material and makes defecation more comfortable; Bufferin 2x 325mg tabs bid (buffered aspirin), which is a nonsteroidal salicylate that inhibits prostaglandin, and also platelet aggregation. It may cause gastrointestinal or gingival bleeding, gastric ulceration, and tinnitus; Maalox 2 tabs tid; which is an antiacid composed of magnesium and aluminum hydroxide.
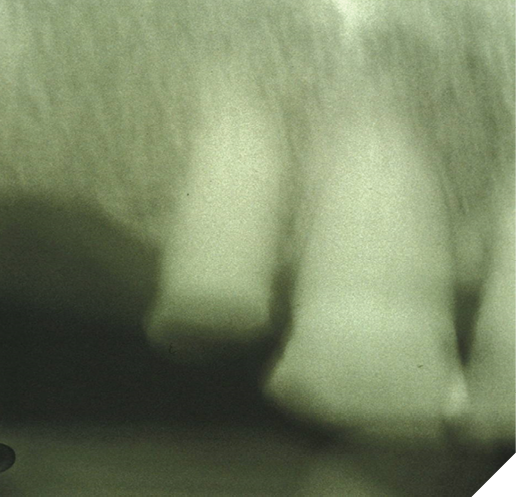
Mrs. MR allowed us to examine her. She had only a limited number of anterior teeth on both maxillary and mandibular arches. The maxillary teeth were #12 to #23, and on the mandibular arch they were #33 to #43, with contact between the arches. All the teeth were worn and #12 was fractured at the gum line and carious. She had a scarred palate where a carcinoma had been removed 3 years ago, and a very dry mouth. She had candidiasis of the palate and angular cheilitis. With the help of her daughter holding her mother’s head, we managed to make an imperfect periapical radiograph of tooth #12 (Fig. 1), which showed a narrowing of the pulp space and no visible periapical radiolucency. It was not possible to determine if Mrs. MR was in pain and she resisted any attempt to pulp test the teeth, as we were unable to communicate with her.
Fig. 1
Considering the information gathered during this limited examination, Mrs. MR would require at a minimum a prophylaxis, treatment of the palatal candidiasis, and either extraction or root canal treatment of tooth #12. Any restorative treatment would only be possible with the use of premedication, using a sedative, such as oxazepam 10mg or lorazepam 1mg one hour prior to treatment. However, when trying to get informed consent Mrs. MR’s daughter refused to give consent for any premedication and/or any type of physical restraint of her mother. We were unable to convince Mrs. MR’s daughter that if she wanted to improve her mother’s oral health, we would need to use some form of chemical or physical restraint.
Considering Mrs. MR’s daughter lack of cooperation, what options were available for the practitioner to address the oral health needs of her mother? The options might include using behavioral modification techniques, such as task breakdown, rescuing, distraction, and bridging.14 Task breakdown consists of dividing the activity in small steps. Rescuing is when a second caregiver takes over the task from the initial caregiver, when the patient reacts negatively to the first caregiver. Distraction uses a favorite item or activity, such as a blanket, a doll, or watching television, to distract the patient while the task is performed. Bridging is having the patient hold an oral care related item, such as a toothbrush, while the provider carries out the treatment.14
For Mrs. MR, behavior modification techniques would be applicable for scaling or cleaning the teeth, and the application of topical fluoride or varnish. However, it would not be adequate for any invasive restorative procedures. Therefore, the patient would need to be restrained physically or chemically, and that would require the informed consent of Mrs. MR’s daughter. Physical restraint in dental care should only be used when necessary for safe and effective treatment, never as punishment or for the convenience of the staff. The least restrictive option must be chosen, ensuring no physical trauma and minimal psychological impact. Its use should be expected to yield reasonable benefits, and both dental treatment and restraint must be consented to. Restraints should be selected based on the specific treatment plan, applied by trained dental staff, and clearly documented—including type, duration, and reason for use.15 If Mrs. MR’s daughter agreed to physical restraint, like an adult papoose board, we would insist that she was in the dental operatory and participate in the procedure, which most caregivers reject.
Therefore, the only other choice to treat Mrs. MR would be to use chemical restraint, which would also require informed consent. However, Mrs. MR’s daughter refused to give us that consent. The only treatment that we were able to carry out was to clean her teeth with a toothbrush, as described by Jane Chalmers,14 in which a toothbrush is bent backward at a 45-degree angle and gently inserted into the corner of the mouth and held firmly against the cheek to help relieve perioral muscle spasms, so that we could remove plaque and debris. Also, we used a syringe to rinse Mrs. MR’s mouth with a chlorhexidine 0.12% solution. To treat her candidiasis, we wrote a prescription for clotrimazole 1% cream (Lotrimin) 15g to be applied to the roof of her mouth and at the angles of her mouth, three times a day, and then NPO for 30 minutes. We do not know what happened with Mrs. MR as her daughter did not respond to any recall or any attempts to contact her.
Final considerations
In geriatric dentistry, informed consent is part of a broader discussion that educates the patient and their caregivers regarding their particular oral health problems, the various treatment options available, which must include risks, benefits, cost, and prognosis, as well as the risk of deciding on the option of not treating the particular problems.11,16
If a guardian, such as Mrs. MR’s daughter, refuses the methods required to treat a patient with cognitive impairment, what should or can the dentist do? Firstly, the guardian should be informed that no treatment may result in increasing amounts of plaque induced oral disease, which may cause local pain and infection and exacerbate systemic problems, such as cardiovascular diseases17 and diabetes.18 Since Mrs. MR lived in a long term care facility, the dentist should show Mrs. MR’s daughter how to brush her mother’s teeth so that she can help to inform the nursing home staff about an appropriate way to achieve adequate daily oral hygiene. As Mrs. MR was non-verbal, it would be important to teach her daughter how to recognize some of the non-verbal signs of oral pain, such as rejecting cold food, pulling at the face and mouth, aggression, and distressed facial expressions.19 There are also many available educational resources to help educate older adults caregivers about oral health care, such as Mouth Care Matters20 and Dental Aging Tips app.21 Additionally, the dentist may suggest a recall schedule which would allow the dentist and the guardian to monitor the progression of the oral disease to be able to intervene as early as possible when a flare-up occurs, such as a periapical or periodontal abscess.
The principles of dental treatment are firstly to eliminate pain and infection, and then to try and improve oral function. If a patient’s guardian refuses to consent to a proposed treatment, which addresses pain and infection, the provider should not be offended but try and seek an alternative approach which allows for monitoring the patient and educating the guardian that if circumstances change, they are welcome to return for care. 
Oral Health welcomes this original article.
References
- Suzman R, Beard JR, Boerma T, Chatterji S. Health in an ageing world—what do we know? The Lancet 2015;385(9967):484-86.
- Banerjee S. Multimorbidity–older adults need health care that can count past one. Lancet 2015;385(9968):587-9.
- Prince MJ, Wu F, Guo Y, et al. The burden of disease in older people and implications for health policy and practice. Lancet 2015;385(9967):549-62.
- Gurwitz JH. The Paradoxical Decline of Geriatric Medicine as a Profession. JAMA 2023;330(8):693-94.
- Marchini L, Ettinger R, Chen X, et al. Geriatric dentistry education and context in a selection of countries in 5 continents. Spec Care Dentist 2018;38(3):123-32.
- Borg-Bartolo R, Roccuzzo A, Molinero-Mourelle P, et al. Global prevalence of edentulism and dental caries in middle-aged and elderly persons: A systematic review and meta-analysis. J Dent 2022;127:104335.
- Ettinger RL, Marchini L. Cohort differences among aging populations: An update. The Journal of the American Dental Association 2020;151(7):519-26.
- Marchini L, Ettinger RL. The Prevention, Diagnosis, and Treatment of Rapid Oral Health Deterioration (ROHD) among Older Adults. Journal of Clinical Medicine 2023;12(7):2559.
- Ettinger RL. “There is nothing wrong with my teeth.” What is informed consent for persons with cognitive impairment? Spec Care Dentist 2002;22(5):172-3.
- Alsaleh A, Kapila A, Shahriar I, Kapila YL. Dental informed consent challenges and considerations for cognitively impaired patients. Periodontol 2000 2021;87(1):43-49.
- Van TT, Chiodo LK, Paunovich ED. Informed consent and the cognitively impaired geriatric dental patient. Tex Dent J 2009;126(7):582-9.
- Mukherjee A, Livinski AA, Millum J, et al. Informed consent in dental care and research for the older adult population: A systematic review. J Am Dent Assoc 2017;148(4):211-20.
- Reid KI. Informed Consent in Dentistry. Journal of Law, Medicine & Ethics 2017;45(1):77-94.
- Chalmers JM. Behavior management and communication strategies for dental professionals when caring for patients with dementia. Spec Care Dentist 2000;20(4):147-54.
- Shuman SK, Bebeau MJ. Ethical issues in nursing home care: practice guidelines for difficult situations. Spec Care Dentist 1996;16(4):170-6.
- Shuman SK. Doing the right thing: resolving ethical issues in geriatric dental care. J Calif Dent Assoc 1999;27(9):693-702.
- Liljestrand JM, Havulinna AS, Paju S, et al. Missing Teeth Predict Incident Cardiovascular Events, Diabetes, and Death. J Dent Res 2015;94(8):1055-62.
- Sanz M, Ceriello A, Buysschaert M, et al. Scientific evidence on the links between periodontal diseases and diabetes: Consensus report and guidelines of the joint workshop on periodontal diseases and diabetes by the International Diabetes Federation and the European Federation of Periodontology. J Clin Periodontol 2018;45(2):138-49.
- van de Rijt LJM, Weijenberg RAF, Feast AR, et al. Oral health and orofacial pain in people with dementia admitted to acute hospital wards: observational cohort study. BMC Geriatr 2018;18(1):121.
- Hartshorn JE, Cowen HJ, Comnick CL. Cluster randomized control trial of nursing home residents’ oral hygiene following the Mouth Care Matters education program for certified nursing assistants. Spec Care Dentist 2021;41(3):372-80.
- Ashida S, Beachy TR, Killian E, et al. An app to support oral hygiene care: Increasing attitudes, knowledge, and confidence in identifying oral health problems among caregivers of persons living with dementia. Spec Care Dentist 2024;44(4):1146-54.
About the authors

Ronald Ettinger, Professor Emeritus, Department of Prosthodontics, The University of Iowa College of Dentistry and Dental Clinics.

Leonardo Marchini, Professor and Chair, Department of Preventive and Community Dentistry, The University of Iowa College of Dentistry and Dental Clinics.
link