

Study design
This article is the second part of a larger mixed-methods study. Initially, qualitative methods were conducted to identify the predictors of medication adherence among elderly individuals with TB. This involved a comprehensive literature review and individual interviews with members of the health care provider team, elderly individuals with tuberculosis, and their family caregivers. Conventional content analysis by Elo and Kingaz (2008) was used to analyze the data. By coding the data and creating subcategories and main categories, variable related to medication adherence were extracted. Subsequently, the Delphi method was used to select and prioritize the most significant variables related to medication adherence in elderly individuals with tuberculosis. Expert opinions were gathered from a diverse group of specialists, including infectious disease and pulmonary specialists, general health practitioners focusing on tuberculosis, tuberculosis nurses, and geriatric specialists. The variables identified during the qualitative phase formed the basis for the current study [20].
The study was conducted at Dr. Masih Daneshvari Specialized Hospital, a renowned center for tuberculosis treatment in Iran. The hospital’s tuberculosis ward consists of 61 general beds and 7 ICU beds. Annually, over 800 patients with tuberculosis are admitted to the hospital, and more than 10,000 patients with tuberculosis or suspected of having it are seen as outpatients [29]. On average, the clinic receives 10 tuberculosis patients and 2–3 elderly individuals with tuberculosis daily from various regions across the country.
The study participants were comprised of elderly individuals and their family caregivers. The inclusion criteria for the elderly participants included being 60 years of age or older, having a confirmed diagnosis of pulmonary tuberculosis, being a new patient with at least one month of treatment, not having cognitive issues as determined by the abbreviated cognitive test [30], being referred to the Tuberculosis and Infectious Diseases Clinic at the hospital, and providing informed consent. Exclusion criteria for elderly patients with tuberculosis were recent hospitalization within the past month, HIV infection, drug-resistant tuberculosis, previous tuberculosis treatment lasting less than 4 weeks, and smear-negative pulmonary tuberculosis patients who had received antibiotics prior to tuberculosis treatment for other conditions. The inclusion criteria for family caregivers of elderly individuals with tuberculosis included having partial or full care responsibilities for an elderly person with tuberculosis for a minimum of 6 months.
Sampling method
Sampling was conducted using a non-random and convenience method. Elderly individuals with tuberculosis and their caregivers who met the inclusion criteria were selected from among those referred to the Tuberculosis and Infectious Diseases Clinic at Dr. Masih Daneshvari Hospital.
Sample size
The variables considered in the conceptual framework of factors related to medication adherence in elderly people with tuberculosis implied 43 manifest variables and 12 latent variables [20]. Additionally, considering a medium effect size (around 0.25), a test power of 0.80, and a type I error of to 0.05, according to the formula provided by Soper for calculating a sample size in structural equation modeling studies [31], the minimum sample size required for the present study was estimated to be 305 people.
$$\begin{array}{c}n=max(n_1,\;n_2)\\\begin{array}{c}n_1\left[50\left(\frac jk\right)^2-450\frac jk+100\right]\\n_2=\left[\frac1{2H}\left(A\left(\frac{\mathrm\pi}6-B+D\right)+H+\sqrt{\left(A\left(\frac{\mathrm\pi}6-B+D\right)+H\right)^2+4AH\left(\frac{\mathrm\pi}6+\sqrt A+2B-C-2D\right)}\right)\right]\\A=1=\rho^2\\B=\rho\;arc\sin\left(\frac\rho2\right)\\C=\rho\;arc\sin(\rho)\\D=\frac A{\sqrt{3-A}}\\H=\left(\frac\delta{z_{1-\alpha/2}-z_{1-3}}\right)^2\end{array}\end{array}$$
Data collection
Data collection took place from October 2022 to February 2023 using a convenience sampling method. To create the general research questionnaire, we first selected important and influential variables from all the variables obtained during the qualitative phase of our study [20]. This selection was based on the opinions of experts in the fields of tuberculosis and gerontology, using the Delphi method. Next, we chose an appropriate questionnaire for each of the desired variables.
The general research questionnaire gathered demographic and background information on the elderly, including age, gender, marital status, education, nationality, residence status, cohabitation status, number of household members, distance from residence to health and treatment centers, employment status, source of income, financial sufficiency, impact of tuberculosis on job and economic status, chronic diseases and medications used, method of obtaining medications, duration of tuberculosis medication use, presence of a treatment supervisor, use of reminder methods, response/non-response to treatment and its effects, side effects of tuberculosis medications, education for patients and caregivers, use of health insurance, use of traditional medicines, motivation for treatment, knowledge about the disease and treatment of tuberculosis, sources of information about tuberculosis, trust in doctors, conditions of treatment centers, and stigma caused by tuberculosis. Additionally, Elderly People with Tuberculosis completed the Morisky, Green, and Levine Medication Adherencequestionnaire(MGL), The Shortened Cognitive Test , The Hospital Anxiety and Depression Scale (HADS) questionnaire, TIPI personality traits questionnaire , The Activities of Daily Living (ADL) questionnaire, The Instrumental Activities of Daily Living (IADL) questionnaire, The Zimet Social Support questionnaire and The Quality of Life questionnaire.
The research questionnaire also gathered demographic and background information on family caregivers, including age, gender, marital status, number of children, education, employment status, financial sufficiency, relationship with the patient, knowledge about the disease and treatment of tuberculosis, sources of information about tuberculosis, and the importance of treating the elderly with tuberculosis from the caregiver’s perspective. The General Health Questionnaire (GHQ) andZarit Caregiver Stress questionnaire were also included.
The questionnaires mentioned above were subjected to psychometric evaluation in Iran. Their characteristics, including validity and reliability, were found to be acceptably sufficient:
The Morisky, Green, and Levine Medication Adherence Scale (MGL) was designed in 1986 by Morisky, Green, and Levine. It consists of four questions that assess the patient’s attitude towards treatment. The answers to the questions are either yes or no. The questions are as follows: (1) Have you ever forgotten to take your medication? (2) Are you careless about the time of taking your medication? (3) Have you ever not taken your medication when you feel better? (4) Have you ever not taken your medication when you feel unwell? A score of zero indicates high adherence, a score of 1–2 indicates moderate adherence, and a score of 3–4 indicates low adherence. The Cronbach’s alpha coefficient of this questionnaire in the field of blood pressure control is 0.61 and has concurrent and predictive validity [32]. This questionnaire has been used as a useful tool for measuring medication adherence in many studies related to chronic diseases [33], including diabetes, hypertension [34], and tuberculosis [34,35,36]. In 2018, Jafari et al. determined the validity and reliability of this questionnaire for elderly people with hypertension, with a Cronbach’s alpha coefficient of 0.86 and test-retest reliability of 0.92 [37].
The Shortened Cognitive Test, first presented by Hodgkinson in 1972 [38], consists of 10 questions. This scale is less dependent on the subject’s level of education compared to similar questionnaires like the Brief Cognitive Status Examination. In 2014, Bakhtiari et al. conducted a study to localize this questionnaire among 176 elderly residents of nursing homes in Iran. The clinical cut-off point for this scale was determined to be less than 8, distinguishing individuals with normal cognitive status from those with mild cognitive impairment. The sensitivity was found to be 92.15%, with a specificity of 81.5%. Internal reliability was assessed using Cronbach’s alpha coefficient, which yielded a value of 0.76, indicating adequate internal reliability [30].
The Hospital Anxiety and Depression Scale (HADS) questionnaire was designed by Sigmund and Snaith in 1983. It consists of 14 questions, with 7 focused on measuring anxiety and 7 on measuring depression. Each question offers 4 possible answers, each assigned a score of 0–3. Score of 0–7 indicate a healthy individual, 8–10 an intermediate individual, and 11 and above a sick individuals [39]. In Iran, Kaviani et al. conducted a study in 2008 to investigate the validity and reliability of the HADS questionnaire in the elderly population. The questionnaire demonstrated face validity, qualitative content validity, and concurrent criterion validity. Reliability was assessed through test-retest analysis, with results showing a correlation of r = 0.75 for the anxiety subscale and r = 0.70 for the depression subscale (both p < 0.001). Additionally, Cronbach’s alpha values were calculated, resulting in 0.85 for anxiety subscale and 0.7 for the depression subscale [40].
The TIPI personality traits questionnaire is a 10-item scale designed to assess personality traits such as extraversion, agreeableness, conscientiousness, emotional stability, and openness to experience. It is a self-reported measure that was created by Gosling in 2003 in the United States based on the Big Five personality theory. The validity and reliability of this scale have been examined [41]. This tool adapted into Persian by Azkhosh et al. in 2019 and validated in the Iranian elderly population. The Cronbach’s alpha coefficient was calcuted to be 0.51 for assessing the internal reliability of the questionnaire, and for the subscales, it ranged from 0.4 to 0.6 [42].
The Activities of Daily Living (ADL) Questionnaire is a tool used to assess the ability of elderly individuals to independently perform daily activities. Katz introduced the ADL index, which consists of 6 items, and demonstrated its validity and reliability. These 6 items include bathing, dressing, toileting, transferring, continence, and feeding. Each item offers two response options: one indicating independence (scored as 1) and the other indicating dependence (scored as 0) [43, 44]. A score of 6 suggests full functionality, 4 indicates moderate impairment, and 2 or lower indicates severe functional impairment [43]. In 2018, Sharifi et al. confirmed the validity and reliability of this questionnaire in the elderly. The study reported adequate validity and an internal reliability of 0.806 using Cronbach’s alpha coefficient [45].
The Instrumental Activities of Daily Living (IADL) questionnaire was designed by Lawton in 1969 to assess instrumental activities of daily living [46]. This instrument has 8 items including telephone use, shopping, food preparation, housekeeping and laundry, transportation, medication management, and money management. The score range is from 0 (completely dependent) to 8 (completely independent). Mirzadeh et al. (2020) determined the validity and reliability of this questionnaire in community-dwelling elderly people. The validity of the questionnaire in this study was found to be adequate and its internal reliability was reported to be 0.96 using Cronbach’s alpha coefficient [47].
The Zimet Social Support Questionnaire, developed by Zimet, Powell, Farley, Workman and Berkoff in 1990 consists of 12 items measuring three dimensions of support from family, friends and significant others. Each dimension contains 4 items, with respondents rating each item on a 7-point Likert scale from 1 (strongly disagree) to 7 (strongly agree). In Zimet et al.’s study, the Cronbach’s alpha coefficients for the significant other, family, and friends’ subscales were 0.91, 0.87, and 0.85, respectively. Item scores range from 12 to 84, with higher scores indicating greater perceived social support [48]. In a 2017 study by Karami et al., the validity and reliability of the Zimet Social Support Questionnaire were assessed in a group of middle-aged and elderly individuals in Kermanshah province. The questionnaire demonstrated adequate validity, with an internal reliability of 0.8 as determined by Cronbach’s alpha coefficient [49].
The Quality of Life Questionnaire (SF-8) is a shortened version of the 36-SF questionnaire, which was developed in the 1980 s by the RAND Corporation and the Medical Outcomes Study (MOS). This questionnaire measures two physical and psychological dimensions, including items such as general health, physical functioning, role limitations due to physical problems, physical pain, vitality, social functioning, mental health, and role limitations due to psychological problems [50]. The subscale scores can be expressed as T-scores (mean = 50, standard deviation = 10), and the range of scores is from 0 to 100. A higher score indicates better health status [51, 52]. The psychometric evaluation of the questionnaire in Iran was conducted by Namjoo et al. in Iranian elderly people with and without diabetes. The questionnaire had adequate validity, with a Cronbach’s alpha coefficient of 0.7 and a test-retest reliability of 0.6 [53].
The General Health Questionnaire (GHQ) was first developed by Goldberg in 1972 and has been widely used to diagnose mild mental disorders [54]. This test consists of 12 items and has two subscales: positive mental health symptoms and symptoms of mental disorder [54]. There are several scoring methods for this questionnaire, with the most common being the traditional scoring method and the Likert scoring method. In the Likert scoring method used in this study, the four options are assigned scores of 0, 2, 1, and 3, respectively [54]. For items related to positive mental health symptoms, the scores range from 0 (much more than usual) to 3 (not at all), and for items related to symptoms of mental disorder, the scores range from 0 (not at all) to 3 (much more than usual). The total score therefore falls between 0 and 36, with a higher score indicating a worse health status [54]. Psychometric testing of the 12-item General Health Questionnaire in Iranian youth was conducted by Ebadi et al. in 2002. The questionnaire demonstrated adequate validity, with a reported Cronbach’s alpha coefficient of 0.87 [55]. Additionally, Namjoo et al. in 2017 examined the validity and reliability of this questionnaire in Iranian elderly people. They found a Cronbach’s alpha of 0.82 and a test-retest reliability of 0.91 [56]. This questionnaire was utilized in the present study to assess the general health status of caregivers of elderly individuals with tuberculosis.
The Zarit Caregiver Stress questionnaire was designed in 1980 by Zarit et al. to assess caregiver stress levels. It consists of 22 items that address personal, social, emotional, and economic stress experienced by caregivers. Each item is rated on a 5-point Likert scale from 0(never) to 4(always). The total score on the questionnaire ranges from 0 to 88, with higher scores indicating a higher caregiver burden [57]. A score of 61–88 indicates severe caregiver stress, 41–60 indicates moderate stress, 21–40 indicates mild to moderate stress, and less than 21 indicates little to no stress. Navidian et al. in 2008, validated the questionnaire through content validity and found strong correlations with the hamilton Anxiety Inventory (r = 0.67) and the Beck Depression Inventory (r = 0.89). The reliability of the zarit questionnaire was also estabished with a test-retest method, yielding a reliability coefficient of 0.94.
Ethical considerations
The present research is part of the PhD course and has been approved by the ethics committee of the University of Welfare and Rehabilitation Sciences with the ethical code IR.USWR.REC.1399.254 in accordance with the Declaration of Helsinki.Necessary permits to conduct this survey were obtained from the university’s research vice-chancellor. The objectives of the research were explained to the participants, and written informed consent was obtained. All subjects were free to participate or withdraw from the study. Patients were informed that their non-cooperation in the study would not affect their treatment process. Additionally, confidentiality of the participants’ information was maintained at all stages of the project.
Data analysis
In the present study, 305 questionnaires related to the elderly with TB and 305 questionnaires related to their family caregivers were analyzed. A significance level of 0.05 was considered for statistical tests. The data analysis of the study was conducted using SPSS-25 software. In the analytical statistics section, independent t-tests, one-way ANOVA, Tukey’s test, Spearman’s correlation test, and ordinal logistic regression model were utilized. In the next step, drawing the structural model, examining the predicted variance of medication adherence and analyzing the direct and indirect effects of the model concepts on medication adherence were also carried out in the Amos environment, using Amos 24.0 software. The initial measurement model showed misfit in residual covariances (e.g., between patient addiction and side effects). Guided by modification indices (MI > 10) and theoretical justification (e.g., shared behavioral barriers like forgetfulness or treatment avoidance), we added correlations between errors of indicators with plausible shared variance. While this improved model fit, we acknowledge that excessive post hoc modifications risk overfitting, which may limit generalizability to other samples. The following fit indices were used to evaluate the overall model: root mean square error of approximation(RMSEA), standardized root mean squared residual(SRMR), comparative fit index(CFI), incremental fit index(IFI), Tucker- Lewis index(TLI), the goodness-of-fit index(GFI), and the adjusted GFI(AGFI). Values greater than 0.90 for CFI, GFI, AGFI, IFI, and TLI, and values less than 0.08 for RMSEA and SRMR indicate an acceptable fit [58].
Findings
The average age of the patients was 72.39 years (± 8.95). 61% of the patients (185 people) were in the 60–75 age group, 37% (113 people) were in the age group of 76–90 age group, and 2% (7 people) were 91 years and older. Additionally, 52.5% (160 people) of the participants in the study were male.
Of the elderly patients with tuberculosis, 44.92% had low medication adherence, 27.54% had moderate medication adherence, and 27.54% had complete medication adherence.
The mean score difference in medication adherence was analyzed based on various categories: personal factors (biological, emotional, behavioral, awareness/knowledge, tuberculosis-related, economic), interpersonal factors (treatment team, family), health service center factors (Organizational factors), and extra-organizational factors (social, health policies). Significant variables predicting medication adherence were included in the model, and the regression coefficient for medication adherence was estimated using multiple rank logistic regression (Table 1).
Based on Table 1, the motivation of elderly individuals with tuberculosis to continue treatment is compared to the baseline of 5.6% for “healthcare team recommendations”. Patients who are motivated by disease remission have significantly lower odds (OR = 0.054) of belonging to higher adherence categories compared to those motivated by healthcare team recommendations. They are 94.6% less likely (1–0.054) to achieve better outcomes than the reference group. Similarly, the group motivated by “Preventing Others’ Infection” (2.3%) has 95.3% lower odds (OR = 0.047) of achieving higher outcomes compared to the reference group. There is no evidence to suggest that family pressure affects outcomes differently than healthcare team advice. Individuals with a more “extraverted personality” demonstrated better medication adherence compared to those with less “extraverted personality“(P = 0.006, OR = 3.9). Patients who used at least one reminder to take their medication showed improved medication adherence compared to those who did not use any reminders (P = 0.004, OR = 3.5). Patients who believed that tuberculosis was a contagious disease demonstrated better medication adherence compared to those who did not hold this belief (P = 0.025, OR = 2.9). Patients whose TB symptoms improved with medication had better adherence to their medication compared to patients whose symptoms did not improve (P = 0.002, OR = 0.1). Patients who did not experience side effects from medication during treatment showed better adherence to their medication compared to those who did experience side effects. (P < 0.001, OR = 0.2). Patients who “trust in the doctor’s knowledge and expertise” showed better adherence compared to those who did not have trust (P = 0.007, OR = 4.2). Regarding the “general health of the caregiver”, for every 1-point increase in GHQ score, the odds of being in a higher adherence category increase by 10% (OR = 1.10), while holding other variables constant. Regarding “patient’s embarrassment about having TB”, patients with low levels of embarrassment have 4.5 times higher odds of being in a higher adherence category compared to those with high levels of embarrassment. Regarding “willingness to disclose tuberculosis”, patients with a “moderate” willingness to disclose have 81.9% lower odds (1–0.181) of being in a higher adherence category compared to those unwilling to disclose (reference). Patients with “high” willingness (6.6%) show no significant difference from the reference group (“None”). In regards to “social rejection of the patient”, patients who do not experience social rejection have 7.5 times higher odds of being in a higher adherence category compared to those who do experience high social rejection (reference). Regarding the Quality of Life Score (QOL), a 1-point increase in QOL reduces the odds of being in a higher adherence category by 14.3% (1–0.857). Regarding the Zimet score, a 1-point increase reduces the odds of being in a higher adherence category by 4.6% (1–0.954).
Based on Table 2, predictors of personal factors, interpersonal factors, organizational factors, and extra-organizational factors were entered into the regression model, respectively. In models 10 and 11, the values of the coefficient of determination obtained from the three statistics of McFadden (0.603), Nagelkerke (0.888), and Cox and Snell (0.849) indicate the high explanatory power of the model by the predictor variables.
To investigate the confirmatory factor analysis and fit of the conceptual model of medication adherence in elderly people with tuberculosis [20], first, the initial measurement model was drawn from the conceptual model (Fig. 1) in the AMOS environment (Fig. 2).
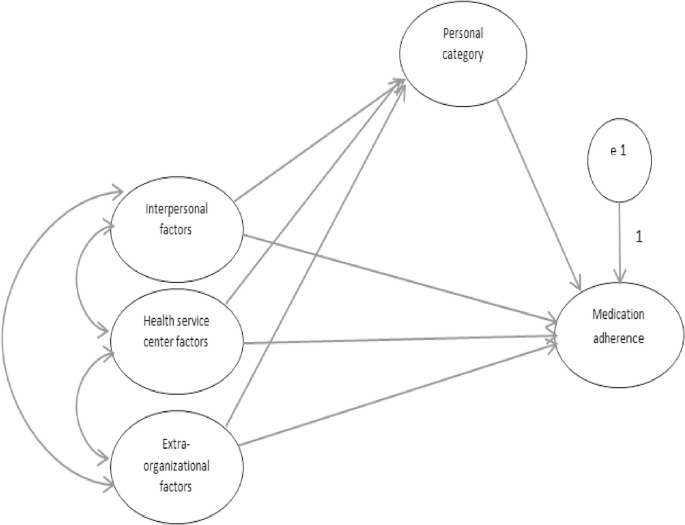
Presents a conceptual model derived from a qualitative study that aims to predict medication adherence [33]

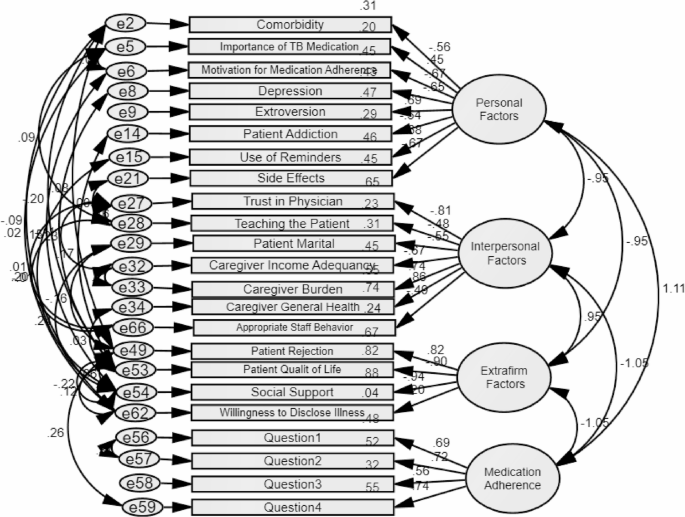
A model for measuring medication adherence in elderly individuals with tuberculosis in the AMOS
After examining the normality of the data, a confirmatory factor analysis model was developed to predict medication adherence using CB-SEM and the generalized least squares method. The model was tested with 5,000 resamples of the sample using the Monte Carlo method (parametric bootstrap) to assess the goodness of fit (Fig. 3).

Model for measuring medication adherence in elderly individuals with tuberculosis
Since the measurement model numbers in Fig. 3 are not legible due to the numerous variables, the correlation matrix between the four classes of the measurement model is displayed in Table 2. Table 3 also provides information on the standardized path coefficients (factor loading with standard beta of the indicators) and their significance levels.
According to Table 3, all four categories of the model exhibit a significant relationship with each other and the level of correlation between categories has been reported to be highly acceptable. Due to the strong relationship between certain variables in different categories, standardized correlation values greater than 1 were observed in the initial model, However, in later stages of model implementation, a two-way relationship was established to adjust the covariances between variables with interacting effects (The information presented in Table 4).
The coefficients of insignificant paths and indicators with a standardized factor loading (or standardized regression weight) of less than 0.5 in Fig. 3 were systematically removed from the model. The model was then re-run, and the coefficients were reexamined as shown in Fig. 4. It is important to note that in Fig. 4 all indicators related to the organizational factor category had weak factor loadings. Leading to the removal of this category from the final model. As a result, in the final model only examined individual factors, interpersonal factors, and extra-organizational factors in relation to medication adherence.

Medication adherence measurement model after removing markers with factor loadings less than 0.5
The initial model presented in Fig. 3 did not have a good fit. In this study, after analyzing the correlation between the errors of the indicators, the goodness of fit of the model was re-examined. The new model (Fig. 5) had good fit indices as shown in Table 5.
Displays the medication adherence measurement model, including some of its key fit indices
In order to investigate the causal relationships between the categories and explain the predicted variance of the outcome variable (medication adherence), a structural model predicting medication adherence was created (see Fig. 6). According to this model, 62% of the variance in medication adherence behavior was predicted by the three categories of the model: personal factors, interpersonal factors, and extra-organizational factors. Additionally, 28% of the variance in the personal category was predicted by the interpersonal factors and extra-organizational factors. The fit indices of the structural model predicting medication adherence can be found in Table 6.
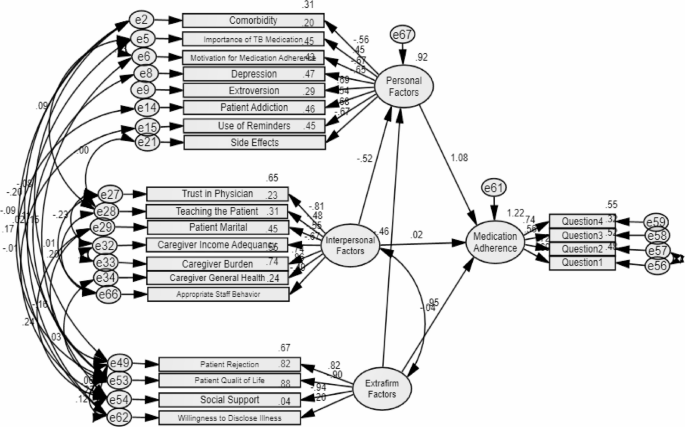
Structural model for predicting medication adherence in elderly individual with tuberculosis, along with the corresponding values of its fit indices
The findings revealed that the standardized regression weight between the concept of interpersonal factors and extra-organizational factors with medication adherence is not significant. However, the standardized regression weight between other concepts of the model and the dependent variable (medication adherence), as well as indicators with factor loading, is significant.
The direct, indirect, and total effects of the study model concepts on medication adherence are presented in Table 7.
Based on the findings in Table 6, the concept of the personal factor category has a significant effect on medication adherence, with an effect size of 0.616. The extra-organizational and interpersonal categories have minor and insignificant effects on medication adherence.
link