

Study design, setting and population
We carried out a retrospective observational study on the entire population of HCWs of the University Hospital (6000 HCWs), all subjected to health surveillance in accordance with Italian laws concerning the protection of workers exposed to occupational risks (D. Lgs. 81/2008), covering a three-year period (1 January 2020–31 December 2022).
The preventive protocol: risk assessment, variables of interest and data collection
A preventive health surveillance protocol was established by the Operative Unit of Occupational Medicine for all HCWs working at the University Hospital of Bari, Apulia, Southern Italy. As required by the protocol, during health surveillance medical visits performed according to Italian law concerning the protection of workers exposed to occupational risks (D. Lgs. 81/2008), all HCWs underwent a physical examination and a measurement of systolic blood pressure (SBP), diastolic blood pressure (DBP) heart rate (HR), height and weight for Body Mass Index (BMI) calculation. BP was measured according to American College of Cardiology/American Heart Association guideline for the prevention, detection, evaluation, and management of high BP in adults17. We used the traditional method of auscultation of the brachial artery with a stethoscope, in either the seated or the supine position, recording BP in both arms and using the arm with the higher reading for subsequent ≥ 2 readings. We used the average of ≥ 2 readings obtained on ≥ 2 occasions to estimate the worker’s BP.
As part of health surveillance medical visits, family, physiological, occupational and pathological medical history were recorded in the health records of each HCW. Furthermore, at the same time, all workers underwent an electrocardiographic examination (ECG) and a blood sampling to evaluate plasma levels of total cholesterol (C-TOT; mg/dL), high-density lipoprotein cholesterol (HDL-C; mg/dL), low-density lipoprotein cholesterol (LDL-C; mg/dL), triglycerides (TG; mg/dL), glycemia (GLC; mg/dL), erythrocyte sedimentation rate (ESR; mm/h), C-reactive protein (C-RP; mg/L), as well as other routine blood indicators (e.g. indices of thyroid and renal function) performed according to the health surveillance protocol for healthcare workers exposed to occupational risk factors. The samples were analyzed at the hospital analysis laboratory using standardized methods and the normal ranges of these parameters were defined according to the sex and age of the worker and to the reference values established by international guidelines and literature data18,19,20,21,22,23.
All workers were classified into four occupational categories, according to the Italian law on occupational risk assessment (D.Lgs 81/08) and to other studies conducted on the same cohort of workers9,24,25,26: physicians, nurses, other HCWs (e.g. biologists, psychologists, healthcare assistants, health technicians, midwives, physiotherapists, medical physicists, childcare workers, orthotists, technicians, students of health professions) and non-healthcare workers (e.g. administrative staff, auxiliary staff, cleaners, drivers, lawyers, librarians, chaplains, doormen, technical workers).
The main CVDs were classified into five categories: rhythm disorders (RD; e.g. tachyarrhythmia, bradyarrhythmia, conduction defects); anatomical-functional disorders (AFD; e.g. anatomical and/or kinetic alterations of the valve structures, of walls and/or cardiac chambers, chronic heart failure NYHA I-IV); ischemic disorders (ID; e.g. ischemic cardiomyopathy, ischemic stroke, stable angina, unstable angina); hypertensive disorders (HD; e.g. grade I, II, III arterial hypertension, isolated systolic hypertension, hypertensive heart disease); other CVDs (OD; e.g. endocarditis, myocarditis, pericarditis, other pericardial pathologies, pathologies of the large extracardiac vessels, peripheral arterial diseases).
Based on the results of the investigations, a risk assessment was carried out, defining HCWs at high risk (HR-HCWs) as subjects suffering from one or more of the following conditions: pathological history of CVDs (e.g. rhythm disorders, anatomical-functional disorders, ischemic disorders, hypertensive disorders, other cardiovascular diseases); alterations identified during the physical examination (PE) of the cardiovascular system (e.g. heart murmurs, rhythm alterations, pericardial rubs, blood pressure alterations); alterations in the ECG performed during the health surveillance examination (e.g. arrhythmias; alterations of the PR interval, QRS, T wave; conduction defects; alterations of ventricular repolarization); new onset of cardiological COVID-19 related symptoms (e.g. dyspnea, chest pain, palpitations, heart murmurs, pericardial rubs). In order to aim for the highest level of prevention, all deviations from normality, even those commonly interpreted as non-pathological (e.g. incomplete right bundle branch block) were considered worthy of further investigation with a specialist cardiological examination, and therefore “at high risk” in reference to our preventive protocol.
All the remaining HCWs were classified as low risk (LR-HCWs). For the latter, no further investigations were necessary and a periodic clinical reassessment was established, outside of data collection for this study. On the contrary, all HR-HCWs underwent a specialist cardiological examination and eventual further diagnostic-instrumental tests requested by the specialist (e.g. echocardiogram, transcranial color Doppler with bubble test, exercise stress test on a treadmill or cycle ergometer, 24-hour ECG recording, myocardial perfusion scintigraphy, cardiac magnetic resonance, coronary angiogram, hospitalization). In case of cardiological examinations negative for CVDs, HR-HCWs were subjected to periodic re-evaluation with a frequency established by the health surveillance protocol, outside of data collection for this study. In case of new onset and/or already known CVDs diagnosis, HR-HCWs were subjected to periodic re-evaluation with a higher frequency, established by the cardiologist.
The health surveillance protocol established by the Occupational Medicine Unit is summarized in the figure below (Fig. 1).
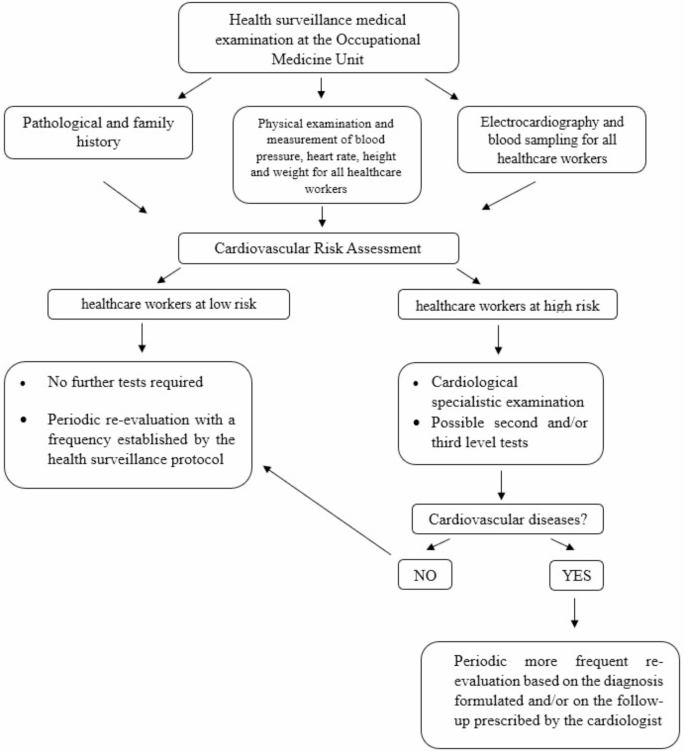
Preventive health surveillance protocol for the management of cardiovascular risk among healthcare workers.
All HCWs were informed that data would be treated in an anonymous and collective way, with scientific methods and for scientific purposes, according to the principles of the Declaration of Helsinki.
Statistical analysis
The analysis was performed using Stata MP18 software. Continuous variables were expressed as mean ± standard deviation and range; categorical variables were expressed as proportions. The normality of the continuous variables was evaluated using the test of Skeweness and Kurtosis, although it was not possible to build a normalization model for those not normally distributed. Continuous variables were compared between multiple groups using the Kruskall–Wallis nonparametric test; categorical variables were compared between groups using the chi-square test or Fisher’s exact test. Multivariable logistic regression was used to evaluate the association between total CVD diagnoses and the different determinants, as well as between new CVD diagnoses and the same determinants. The adjusted odds ratio (aOR) was calculated, with the 95% confidence interval (95% CI) indicated. The Pearson’s chi-squared test was used to evaluate the goodness-of-fit of multivariate logistic regression models. For all tests, a p-value < 0.05 was considered statistically significant.
Statements
The patients were informed that data from the research protocol would be treated in an anonymous manner based on scientific methods and for scientific purposes in accordance with relevant guidelines and regulations and with the principles of the Helsinki Declaration.
Ethical approval was not necessary because all medical and instrumental examinations were performed according to Italian laws concerning the protection of workers exposed to occupational risks (D. Lgs. 81/2008). Nevertheless, the study was approved by the Ethics Committee of Azienda Ospedaliero-Universitaria Consorziale Policlinico of Bari (Parere Studio N. 7241).
Informed consent was obtained from all subjects involved in the study.
link